Engineering a Healthier Future
UB neurosurgeons innovate powerful new ways to attack multiple blood clots deep in the veins of the brain

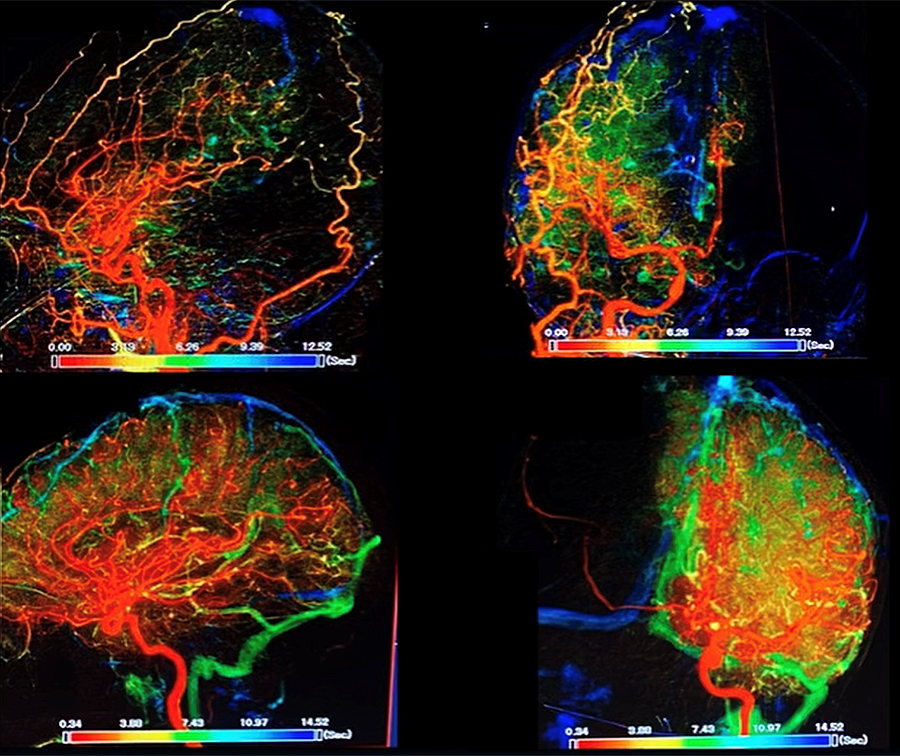
These images show the arteries (red) and veins (green) in the brain of a recent patient with CVST. Before surgery (top images), the arteries (red) are the dominant color but the veins (green) are hard to see because they are so severely occluded. After surgery (bottom images), the veins (in green) are clear, not occluded and are easy to see. Credit: UB Neurosurgery.
At Gates Vascular Institute, the UB team is developing new approaches to address rare events that can strike young people, sometimes after COVID-19 infection
Release Date: September 14, 2022




{kind=link}
BUFFALO, N.Y. – The University at Buffalo team that a decade ago helped usher in a new era in acute stroke treatment has turned its innovative approach to addressing the rare but potentially deadly phenomena when multiple blood clots strike deep in the veins of the brain.
“Typically, when we think of stroke, we think about blockages in the arteries to the brain,” said Elad Levy, MD, SUNY Distinguished Professor, L. Nelson Hopkins Chair of Neurological Surgery and chair of the Department of Neurosurgery in the Jacobs School of Medicine and Biomedical Sciences at UB. “But blockages can also happen in the deep veins of the brain.”
The condition is called cerebral venous sinus thrombosis (CVST), where a blood clot forms in the brain’s venous sinuses, preventing blood from draining out of the brain.
“In these very rare cases, when multiple veins are involved, the blood coming into the brain can’t drain out,” Levy said. “This causes the brain to swell in the skull, which can lead to hemorrhage.”
When a single clot in the brain is involved, the standard of care is to treat the patient with blood thinners. But, Levy said, cases of multiple clots in the veins of the brain require a more aggressive approach.
“If the patient falls into a coma, then you need to act fast and mechanically pull those clots out of the brain veins,” he said. “The faster you get in there to open up the vessels, the better the patient will do.”
When multiple major veins in the brain are obstructed, a phenomenon the UB team has seen more than a dozen times since 2009, including recently with COVID-19, the neurosurgeons have used mechanical thrombectomy to literally suck the clot out of the vein. The procedure is called venous thrombectomy.
“Venous thrombectomy is not truly standardized yet,” said Rosalind Lai, MD, who recently joined UB Neurosurgery as a fellow after completing her medical education at Harvard Medical School and residency at Brigham and Women’s Hospital. “There’s still active research into when and how it can be helpful for patients.”
And while Levy stressed that these phenomena are exceedingly rare, the UB team has treated two such cases in the past month in young, otherwise healthy individuals who had recently been infected with SARS-CoV2.

Image shows the catheter (skinny black line in the middle of the skull) a tube that was threaded through the patient’s femoral vein in her leg and up into her skull. The black line is the wire that guides the catheter to get up to the top of the head, in order to suck the clot out of the vein. Credit: UB Neurosurgery
{kind=link}
One of those patients continued to rapidly decline, even after several hours on a blood thinner.
“In that case, we really had no choice but to do the procedure,” said Lai, who assisted Levy in the operation. “The procedure went really smoothly. Dr. Levy is beyond words in terms of what he can do. He got in there very quickly and took the clot out.”
After the procedure, CT images showed that all the occluded veins had been opened up.
“And clinically, over the next few days, the patient continued to improve,” said Lai. “It was remarkable to see how this procedure made for such a life-changing event for this individual. Her case shows that there’s a definite need for more study on indications for venous thrombectomy. We need to be good at selecting the right patients for the procedure. She was certainly a great candidate for this.”
The next frontier
“This is the pivot point with stroke,” said Levy. “Learning how to treat vascular disease from the venous side versus the arterial side is the next frontier.”
It’s a frontier that the UB team is well-suited to explore.
“Whether it’s finding ways to expand the time window for treatment or adapting techniques from other disciplines, the mission of the UB Department of Neurosurgery has been to explore powerful innovations that will help more patients get back to normal life and function,” said Allison Brashear, MD, vice president for health sciences at UB and dean of the Jacobs School.
Led by L. Nelson “Nick” Hopkins, MD, SUNY Distinguished Professor and former chair of the UB Department of Neurosurgery, the team began pioneering new techniques back in the 1990s, using minimally invasive stroke treatments. These treatments take advantage of the body’s circulation system by threading micro-thin devices through an artery in the groin to reach blocked vessels in the brain, where they are then treated with stents.
Despite initial resistance to those innovations, the field has embraced them. Mechanical thrombectomy to remove arterial clots is now the established standard of care for certain types of acute stroke. The UB team is now using a similar minimally invasive approach to treat multiple blockages in the veins of the brain.
That mindset, focused on finding more ways to intervene even in the most severe situations, is again at work with the CVST cases, said Levy, who completed his fellowship under Hopkins in 2003, joined the UB faculty in 2004 and was named chair of neurosurgery in 2013.
“The ethos, the culture among UB neurosurgeons, is to push the envelope, to expand the landscape of stroke intervention, to develop and implement novel technologies to continue to provide cutting-edge care for increased patient populations,” said Levy, who is president of UBNS, the neurosurgery practice plan of UBMD Physicians’ Group.
Over the past dozen years or so, at Kaleida Health’s Gates Vascular Institute, where Levy is co-director of the Gates Stroke Center and Cerebrovascular Surgery as well as director of endovascular stroke treatment, he and his team have treated 20 cases where blockages occur in many or even all of the major veins of the brain. Some of these cases involved otherwise healthy young people, some of whom were recovering from COVID-19.
While the connection with COVID-19 is not yet clear, the UB researchers expect their ongoing studies of these clots and their access to those stored in UB’s Clinical and Translational Research Center biorepository will provide insights into how and why they occur.
Multidisciplinary endovascular expertise
Strong collaborations with the Endovascular Devices and Imaging Lab in the Canon Stroke & Vascular Research Center, located upstairs from the GVI, provide the neurosurgeons a critical tool in exploring how to treat endovascular disease including CVST.
Led by Ciprian N. “Chip” Ionita, PhD, assistant professor of biomedical engineering in the School of Engineering and Applied Sciences and the Jacobs School, the center focuses on creating 3D-printed phantoms of the body’s complex circulatory network so that surgeons can optimize their procedures before they head into the operating room.
“We subject all the devices to different patient anatomies in 3D-printed phantoms to see which one is better for a particular task,” he explained. “You can evaluate them in animal models but those don’t give you the ability to experience human anatomy, which can be very different in some people. There are these very tortuous pathways that have to be navigated all the way to where the clot is. You need to optimize the techniques in order to pull out those clots.”

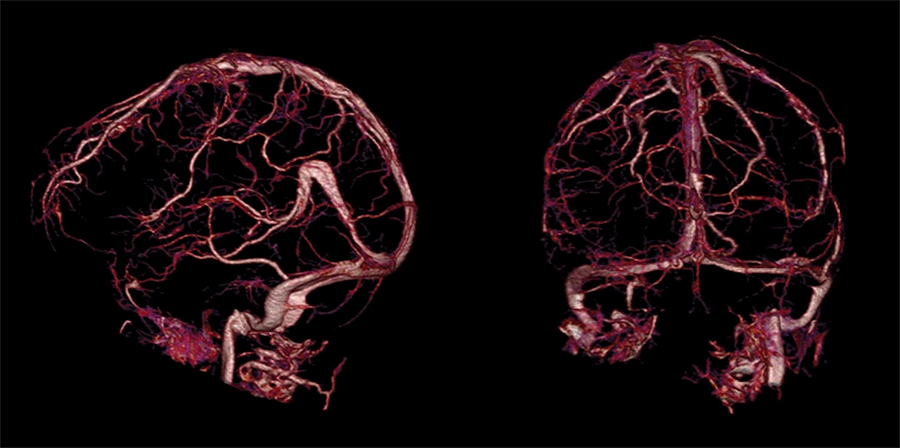
After the procedure, all the veins (shown in pink and red) are open and visible. Credit: UB Neurosurgery
{kind=link}
Advances in the stents themselves are also playing a role, advances that in some cases are a direct result of the collaboration the UB team at the GVI has with the Jacobs Institute (JI), a nonprofit organization whose mission is to accelerate the development of next-generation technologies in vascular medicine.
The JI is located just upstairs from where the UB neurosurgeons perform the surgeries in the GVI/CTRC building that was specifically constructed to promote these kinds of collaborations between scientists, engineers and surgeons.
“We work very closely with the research engineers and scientists at the JI to provide feedback from these cases in real time,” said Levy, “so engineers can continue to work with the device companies to create second- and third-generation devices, making them bigger, longer and more supple.
“The technology is evolving, so now we can get bigger tubes farther and deeper into the brain,” Levy continued. “Stents are being made out of novel polymers, which allows them to be more flexible so they are better able to navigate and wind around the twists and turns of human vascular anatomy.”
Suction catheters are now as wide as the circumference of a pen or even a marker, Levy explained, which in some cases is double the diameter of earlier devices, making them much more powerful.
“The bigger the tube the greater is the suction power to get these massive clots out of there,” he said. “There is a lot of science and technology advancing these tools for stroke intervention. Now we are taking them to use them on the venous side, but they weren’t developed for this. We borrowed them from cardiology and other disciplines, and are adapting them.
“Our decades of experience in thrombectomy and in brain venous anatomy coupled with the sheer volume of neurointerventions that we do has resulted in UB Neurosurgery and the GVI becoming a center to which hospitals around the world refer their patients suffering from complex neurovascular disease,” said Levy.
Media Contact Information
Ellen Goldbaum
News Content Manager
Medicine
Tel: 716-645-4605
goldbaum@buffalo.edu